I became a blogger 4 months ago, a gig that I find fascinating and refreshing. A place for me to vent, pontificate, and generally hold forth with a jaundiced view of my profession and the industrial Goliaths that support it.
News
Sen. Joe Lieberman is officially working to block health care reform in the Congress; he especially desires de-postponing any kind of "health care reform" until the economy has recovered.

Arthritis of the cricoarytenoid joints is not as rare as is commonly believed. Many sources still consider cricoarytenoid arthritis to be an atypical symptom of rheumatoid arthritis in spite of evidence to the contrary.
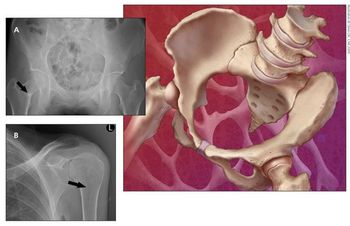
ABSTRACT: MRI allows for earlier detection of the joint synovitis, erosions, and bone marrow edema present in inflammatory arthritis, facilitating earlier diagnosis and treatment.
The vasculitides are a heterogeneous group of disorders characterized by inflammation and necrosis of blood vessel walls resulting in impaired blood flow and organ damage. This article addresses some of the most frequently asked questions about these conditions.
Better understanding of meniscus anatomy and function has triggered a search for new and improved treatment options. Nonoperative treatment, including activity modification, rehabilitation, and use of NSAIDs, is directed at minimizing symptoms of pain and swelling.
The prevalence and extent of vascular calcification over the thoracic aorta and coronary and carotid arteries are greater in patients with systemic lupus erythematosus (SLE) than in healthy persons. Because the process of atherosclerosis related to SLE disease activity is diffuse and widespread rather than limited to the coronary arteries, coronary calcification used alone as a marker for atherosclerosis may not disclose the association.
Large organizations with mobile workers, such as hospitals, face diminished productivity when communication is inefficient and its employees are unable to locate their coworkers in a timely manner.
For those interested in health information technology, there is now an excellent, new, powerful website about this topic called the Huffington Post Investigative Fund. In their most recent report, "Can Cleveland Clinic Be a Model for Digital Medicine?" they discuss how this hospital system has failed to recoup their $100 million investment to date.
Lately, I've been thinking about how fast everything moves these days. This is true in technology, medicine, business, and other important areas of our lives. Keeping up with changes in healthcare is a real challenge; just reading monthly print medical journals won't cut it anymore in the digital age. Now, practically every day I find myself looking something up on Wikipedia.
The powerful vendor-lobbying group, HIMSS, has been extremely successful over the last 8 years lobbying our elected political leaders about HIT.
I have been following with interest all the discussions about the new Medical Home (aka, the Patient Centered Medical Home) concept. This is our silver bullet that will improve patient access, raise quality levels, increase overall satisfaction and save billions of healthcare dollars - all at the same time!
Obesity is a modifiable risk factor for knee osteoarthritis (OA). Weight loss may reduce the risk of knee OA, and increased levels of physical activity may result in improvements in disability-related outcomes. However, intensity of physical activity is not as important in weight loss as total energy expended.
Pulmonary arterial hypertension (PAH) may lead to increased pulmonary vascular resistance, compromised vasoreactivity, right heart failure, and death. PAH, a subset of pulmonary hypertension (PH), classically is associated with systemic sclerosis but also occurs with other rheumatologic conditions. Early diagnostic strategies are essential. The symptoms of PAH often are nonspecific; the most common presenting symptom is dyspnea.
Older patients experience shoulder pain more frequently than younger patients and present with different issues. Using a combination of tests with a detailed history is the best approach to narrowing the differential.
Contrary to earlier reports, mineralization of articular cartilage is a common event in end-stage osteoarthritis (OA) and is closely associated with disease progression. There is a significant correlation between clinical symptoms and the amount of mineralized cartilage.
The jump protocol with analysis of time to stabilization (TTS) can discriminate between persons with and those without functional ankle instability (FAI), according to researchers in the Department of Sport and Exercise Science at the University of Auckland in New Zealand. Persons with FAI have delayed trunk muscle reflexes to a sudden perturbation, supporting theoretical and experimental descriptions of proximal adaptations associated with ankle injury.

A new network from the University of Alabama at Birmingham (UAB) will create a national database that aims to see how rheumatoid arthritis (RA) patients respond to different RA drugs, and then use that information to further personalize RA treatment.
Among the numerous posters on display under the "Fibromyalgia and Soft Tissue Disorders" heading on day 4 at the American College of Rheumatology/Association of Rheumatology Health Professionals 2009 Annual Scientific Sessions were posters focused on the development of a fibromyalgia (FM) responder index, anxiety and depression among patients with FM, tai chi as an effective treatment of FM, and sex differences in predictors of increased symptoms after exercise and sleep restriction in patients with such chronic pain disorders as fibromyalgia.
Dozens of posters were presented under the RA umbrella during the morning of day 4 at the American College of Rheumatology/Association of Rheumatology Health Professionals 2009 Annual Scientific Sessions.
Dozens of posters were presented under the "Fibromyalgia and Soft Tissue Disorders" umbrella during the morning of day 4 at the American College of Rheumatology/Association of Rheumatology Health Professionals 2009 Annual Scientific Sessions. Among the highlights are the following.
The 2009 American College of Rheumatology/Association of Rheumatology Health Professionals Scientific Meeting will feature several “Curbside Consult/Ask the Professors” sessions. Designed to feature information and discussion about “difficult management decisions that must be made in the absence of strong data,” these sessions give attendees the opportunity to “compare their personal management approaches” to the clinical problems outlined in the featured vignettes and scenarios with those of “the academic expert consultants and other clinicians in the audience.”
A new study finds that pindolol is highly effective for the treatment of fibromyalgia symptoms manifesting themselves through the autonomic nervous system.
Researchers examining senior-identified arthritis management strategies were able to identify the most helpful treatment methods as well as the biggest challenges preventing most seniors from engaging in these practices.
Despite findings from other studies indicating that somnolence is a sometimes significant adverse effect in pregabalin use, this study suggests that it is statistically insignificant.
RA patients identified through the Department of Veteran Affairs national administrative databases that were on anti-TNF therapy had a higher risk of developing non-melanoma skin cancer than those on non-biologic DMARDs.
Fibromyalgia syndrome (FMS) is characterized by widespread chronic pain and tenderness. Persons with FMS are a diverse population, with widely variable symptom presentation and severity, as well as secondary symptoms. Because the symptoms are so diverse, diagnosis and management become challenging. Mounting evidence supports altered CNS processing of nociceptive stimuli as a mechanism.
As the population ages and persons live longer with more medical comorbidities, the incidences of both gout and pseudogout will continue to increase. Uric acid metabolism is crucial to the pathogenesis of gout. Patients who have the arthritis associated with crystal-deposition disease typically present clinically with acute attacks of joint pain, swelling, and erythema and have asymptomatic periods between acute attacks.
Clinical study findings of recent years support the notion that patients with rheumatoid arthritis (RA) should be treated earlier and more aggressively. Monotherapy with disease-modifying antirheumatic drugs (DMARDs) is effective in some cases, but triple DMARD therapy is superior to double therapy or monotherapy in early or late RA. Leflunomide is at least as effective as methotrexate (MTX) and sulfasalazine and more effective than placebo.
A disruption in any part of the vitamin D physiological pathway can result in vitamin D deficiency, which may lead to bone pain, muscle weakness, falls, low bone mass, and fractures.
Advertisement
Advertisement