SLE is an unpredictable and often confusing disease that affects more than 1.5 million Americans and at least 5 million persons worldwide.
News
The Disease Activity Score 28 (DAS28) values for patients with rheumatoid arthritis (RA) vary considerably with their perception of pain and their sex.
Injectable corticosteroids may be used for managing painful shoulder conditions, but there are no universally accepted guidelines for dosage and administration. Understanding the mechanisms of action is critical for knowing when they can be used effectively. The biggest absolute contraindication to intra-articular or extra-articular corticosteroid injections is evidence or probability of infection. Relative contraindications include anticoagulation therapy, hemarthrosis, and poorly controlled diabetes mellitus. Most complications result from frequent use and can be avoided with appropriate doses and dosing intervals. Intra-articular and periarticular corticosteroid injections may cause significant systemic effects. The misuse of corticosteroid injections often is overuse. Creation of uniform guidelines for injections would help reduce their deleterious effects and maximize pain relief. (J Musculoskel Med. 2008;25:78-98)
<em>The outlook for patients with newly diagnosed rheumatoid arthritis (RA) has improved greatly, but many questions remain, including when to initiate therapy and what drugs to use. Recently issued recommendations for managing early RA include referring patients who present with arthritis of more than 1 joint to a rheumatologist. Combination's of drugs have been shown to be more effective than monotherapy. The tumor necrosis factor α inhibitors have revolutionized treatment, and other biologic agents are available for those who have an inadequate response. Making the diagnosis early often presents a challenge. Recently, a prediction rule was published for patients with undifferentiated arthritis of recent onset. The imaging focus for early arthritis has shifted from radiographs to ultrasonography and MRI. (J Musculoskel Med. 2008;25:70-76) </em>
Elbow fracture-dislocations are complex injuries that encompass both soft tissue and bony injury. Recognizing the significance of the bony articulation, soft tissue complex, and support of the musculotendinous units is central to an understanding of the pathoanatomy. Four common patterns have been identified, 2 that are true dislocations with loss of ulnohumeral articulation and 2 that represent only an ulnohumeral disruption but warrant inclusion as elbow fracture-dislocations. Complications may be early (eg, instability and stiffness) or late (eg, arthrosis). Three anatomical components provide stability and facilitate elbow function: the osseous articulation, capsuloligamentous complex, and musculotendinous units. With each progressive stage of soft tissue injury, the elbow experiences increasing instability. Elbow fracture-dislocations require operative treatment. (J Musculoskel Med. 2008;25:53-62)
The number of persons with arthritis or another rheumatologic condition is expected to climb to 67 million-a whopping 44% increase-by the year 2030, according to a new study released by the CDC for the National Arthritis Data Workgroup (NADW). The prevalence of osteoarthritis, the most common form of arthritis, has increased to about 27 million persons, up from an estimated 21 million in 1990, showing a 29% increase. Gout now affects about 3 million adults, representing a 43% increase. Of all the common rheumatologic conditions, only rheumatoid arthritis (RA) has decreased in prevalence (Table).
Persons who engage in intensive computer keyboard use in the workplace are at lower risk for carpal tunnel syndrome (CTS) than those who do not. Keyboard use actually may be protective because repeated low force muscle activity may decrease the risk of edema and increased tissue pressure.
The spondyloarthropathies (SpA) are strongly associated with the HLA-B27 gene. The diagnosis is based primarily on clinical findings. Ankylosing spondylitis (AS) often involves the sacroiliac joints and spine. Psoriatic arthritis (PsA) occurs in up to about one third of patients with psoriasis. Reactive arthritis must be distinguished from other arthropathies. Arthritis occurs in about 30% of patients with inflammatory bowel disease. Undifferentiated SpA include sseveral related disorders. Radiographic evidence of sacroiliitisis a characteristic feature of AS. SpA management should include patient education and regular exercise. NSAIDs are the first line of treatment.The tumor necrosis factor α inhibitors are highly effective inpatients with active AS and in those with PsA that is unresponsive to conventional therapy. (J Musculoskel Med. 2008;25:31-40)
Laboratory findings, diagnostic methods, and best treatments for giant cell arteritis, a major cause of vision loss and other health problems.

Involving patients in decision making may help improve the quality of care.
Increasing physical activity has proved effective in improving patients’ overall health and preventing and managing chronic diseases and complications, such as obesity, coronary artery disease, diabetes mellitus, arthritis, and osteoporosis.
Young-Min S, Cawston T, Marshall N, et al, Queen Alexandra Hospital, Portsmouth, UK, and other centers. Biomarkers predict radiographic progression in early rheumatoid arthritis and perform well compared with traditional markers. Arthritis Rheum. 2007;56:3236-3247.

He had bilateral hand pain. History included rheumatic fever, aortic valve replacement, corticosteroid-induced osteonecrosis, and total left hip arthroplasty.
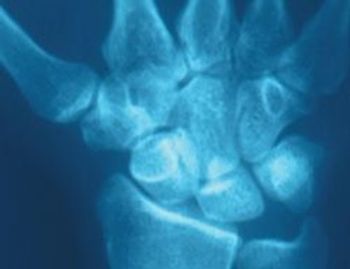
She caught herself with her hands in a forward fall. A year later, her wrist is still painful. What should be done?
A 79-year-old white woman presented with ulcerative colitis of 12 years’ duration and osteoporosis. She was referred to rheumatology for severe proximal muscle pain that was unresponsive to NSAID therapy.

A 29-year-old African American woman came to our rheumatology clinic with right hip pain that had been getting worse for the past 3 months. She had been diagnosed with systemic lupus erythematosus (SLE) 2 years earlier. She reported excruciating right hip pain and mild pain in her left hip on weight bearing and, occasionally, at rest.

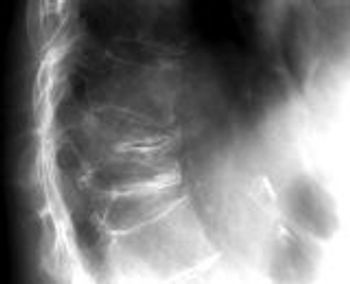
A 48-year-old woman presented to the orthopedic clinic with dull, persisted pain in the sacroiliac area that was impervious to NSAIDs. She denied knowledge of any injury or other possible explanation.
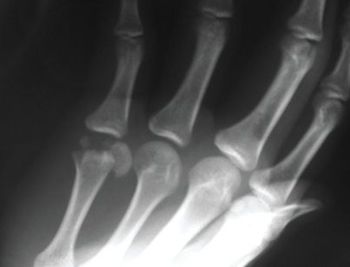
An 18-year-old complained of pain and decreased mobility of the small finger in his right hand after a softballinjury. While sliding back to second base during a pickoff attempt, the patient hit his hand on the bag.

A 55-year-old American Indian truck driver presentedwith a 2-day history of right wrist swelling and pain. He denied previous trauma to the wrist or having performed unusual activities.

A 63-year-old woman presented with a 2-year history of bilateral hand pain and stiffness that had worsened in recent months. The pain was most severe in the fingers and was associated with morning stiffness that lasted 30 minutes. There was loss of full range of motion in some finger joints.

A 51-year-old African American man with a 15-year history of chronic hepatitis C and sarcoidosis presented with persistent bilateral hand pain. The pain was aggravated by physical activity and had a waxing-and-waning pattern.

A 56-year-old man presented with a 1-week history of digital tip ulcers and ischemic gangrene. He alsoreported the recent onset of Raynaud phenomenon and diffuse joint pain.
Advertisement
Advertisement