







































































For patients diagnosed with systemic lupus erythematosus (SLE) finding relief for their symptoms can make a large difference in their quality of life.
Lupus
Latest News

Advertisement
CME Content
Advertisement
(ACR2014) Another Rheumatology Network Editorial Board member weighs in: Christopher Collins MD saw reason for great encouragement in a report about an interferon-α blocker for systemic lupus erythematosus.
(ACR2014) A team from Rush University says their new 10-point instrument developed should be useful to track lupus disease status for trials and in the clinic.

(ACR2014) Early comparisons of patients with rheumatic disease who use marijuana with those who don't show that the practice is not associated with better pain relief. But it is associated with some "sobering" consequences.

Doctors treating a patient for a lupus flare presenting as a fever were puzzled when her body temperature suddenly plunged. After solving the problem, they learned that it is rare but not unique -- and may be somewhat predictable.
This 14-year-old girl not only has lupus; she has also been diagnosed with arthritis, a vasculitic rash, and myositis. Can you guess what's actually going on here?

Nausea and vomiting are the first symptoms of lupus in these three case studies. The consequences of misdiagnosis can be life-threatening.
Already discontinued for rheumatoid arthritis, the candidate drug tabalumab will no longer be tested for lupus either. Observers are taking a positive view of the situation.

Trials of tabalumab showed "insufficient efficacy."
People who have rheumatoid or psoriatic arthritis or lupus are at increased risk for shingles. Studies suggest that treatment for the rheumatic condition may be a factor in certain circumstances.

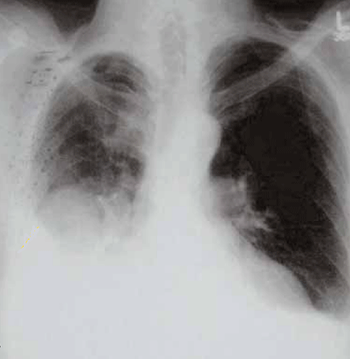
Confirming the high pneumonia risk in lupus patients, researchers in Spain have found that it may precede the onset of the immune disorder. Their biological studies suggest that a particular underlying immune abnormality may explain both.

Reasons why women with lupus change from azathioprine to mycophenolate mofetil or vice versa are different, as is the success of switching.
The first step in reducing the burden of infection during lupus nephritis is understanding where and how it happens.

The patient is plagued by problems: Severe headaches, nausea, vomiting, a rash, chest and abdominal pains, and by the time she reaches a rheumatologist, periorbital edema and photophobia. Can you guess the cause?
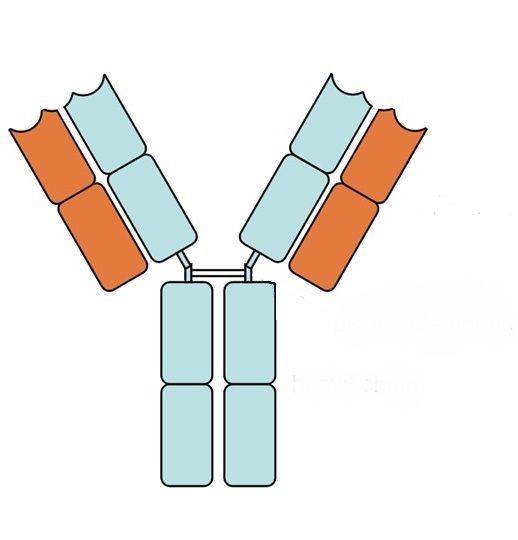
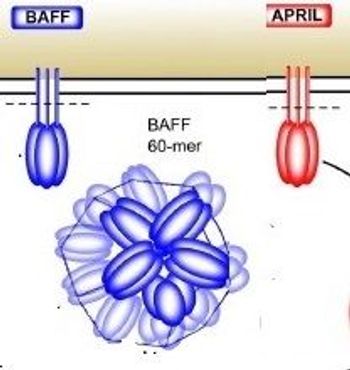
Last year's approval of belimumab (Benlysta) revolutionized lupus treatment. How safe and effective is it, actually? Do similar inhibitors of the B-cell activating factor BAFF, now in testing, appear even more promising? Here are the basics from an expert on the subject.
Researchers found a more than tripled risk of ASDs and VSDs in children born to SLE mothers in a study reported at the recent annual meeting of the American College of Rheumatology.
In partnership with the British Medical Journal, the Lupus Foundation of America will publish Lupus Science and Medicine beginning in 2014.
ACR2013: Joints erode in systemic lupus erythematosus and primary Sjӧgren’s Syndrome. But French researchers say their MRI studies don't justify classing them as erosive disorders like rheumatoid arthritis.
ACR2013: Retrospective analysis of more than 10,000 pregnancies documents increased risks for hypertension, preeclampsia, preterm delivery and stillbirths among women with SLE.
ACR 2013: Stymied by high response rates in the "usual care" comparison arm of new-drug trials, lupus researchers are testing a bold idea: Carefully withdraw treatment from the control group.
ACR2013: As well as neonatal lupus and heart block, new research suggests that children born to women with lupus may face higher risks for autism and attention deficit hyperactivity disorder.
ACR2013: More familiar as a suspect in Alzheimer disease, amyloid proteins may trigger autoantibodies in lupus when introduced via infection, a mouse study suggests.
Last week the major British journal published an exhaustive series of reviews on autoimmune rheumatic disease, summarized briefly here. Also new in the nonspecialty journals: Macitentan for pulmonary hypertension, small fiber neuropathy in Sjögren syndrome, and risk factors for infection with glucocorticoids.
A 45-year-old woman presented with longstanding left knee pain. Both knee and hand radiographs showed abnormalities. Bony infarcts had become complicated by an infection/septic joint and had progressed to frank bony destruction.

Dr. Lim discusses the challenges of diagnosing and treating lupus, the tools and resources offered by the Lupus Initiative, and the impact of unconscious bias on care.
Advertisement
Advertisement